HistoryRemember to check left or right -handed ness, occupation, and social situation
DocumentationRefer to fingers by name not number.
Use palmar (or volar), dorsal, radial, ulnar (not anterior, posterior, lateral, medial).
Document important positives, as well as important negatives
ExaminationRemove rings as soon as possible
X-ray if any likelihood of glass
ElevationThe importance of elevation can not be emphasised enough. The injured hand must always be higher than the heart. Many complications from hand injuries are not from the fracture and associated soft tissue, but from persistent oedema - making healing slower, and surgery more difficult. Elevate!
HealingA fracture in the hand takes 4 weeks to heal clinically, and is faster in children. Radiographic healing can take 4 - 6 months. They begin to heal 7 days after injury. Attempts at closed manipulation after 7 days in children, and adults in 10 days are usually unsuccessful.
Hands should be seen by the specialist less than 5 days after the initial injury.
Tendon InjuriesExtensor Tendon Injuries: Plastics Extensor tendon injuries can be just as devastating as flexor tendon injuries. If suspected, whether partial or full, refer the patient to plastic surgeons. If the injury is less than 50%, conservative management may be considered. A mallet splint should be applied, even if no deformity is apparent.
A mallet finger is loss of extensive extension of the distal interphalangeal joint caused by failure of the terminal slip of the extensor mechanism at its insertion. It is often caused when the extended finger is accidentally stubbed against a hard surface. They should be x-rayed to see whether there is an avulsion fracture present - bony injury is a good prognostic indicator.
Large bony fragment (>1/3 articular surface) = mallet splint + speedy plastics review.
No bony fragment = plastics review clinic 7 - 10 days
Subluxation = speedy plastics review
Flexor Tendon Injuries: PlasticsThere is some controversy about whether to repair these or not. Lacerations can cause flexor tendon injuries, and avulsions from the base of the distal phalynx are commonly missed.
“Rugby shirt finger” is more common in adolescence, and commonly affects the ring finger. Forced extension of the distal phalanx (as in grabbing someone’s collar at rugby) tears the FDP tendon. They can be difficult to diagnose, and a high index of suspicion from the history is needed. They require surgery in <10 days.
Ulnar Collateral Ligament: Plastics The UCL can be ruptured by forced abduction - nowadays from falling when skiing onto the ski-pole. It used to be caused by gamekeeping injuries. The eponymous name “Gamekeeper’s thumb” is being replaced by “Skiiers thumb”. Complete rupture is when the two parts of ligament being separated by the adductor aponeursis (the Stener lesion”).
UCL Sprains: Sometimes the UCL is sprained, and it can be difficult to assess for laxity due to pain. Some texts suggest anaesthetising the UCL and re-assessing. If you are unable to assess the UCL and have a high index of suspicion, treat as per rupture and refer the patient to plastics clinic follow up. If you are unable to assess the UCL and have a low index of suspicion, refer the patient to UCC follow up clinic.
UCL Laxity: If there is laxity >30 degrees, refer the patient to plastics. The thumb should be immobilised in thumb-spica - either tape or plaster of paris.
Avulsion fracture: a UCL sprain or rupture + avulsion fracture should be treated with a scaphoid plaster of paris, and plastics referral.
Nerve InjuriesDigital Nerve Injury: PlasticsThe digital nerve can easily be damaged, and often sensation is intact, but altered. Complaints of altered sensation should be taken seriously.
It is important to have sensation over the edges of the hand - the thumb, the radial aspect of the index finger, or ulnar aspect of the little finger. Repair can be successful up to 2 weeks after injury.
The digital nerves can be repaired up to the level of the DIPJ, although it may be decided not to repair injuries distal to the PIPJ.
When examining the finger for suspected digital nerve damage, it can be useful to test for tactile adherence by running a bic biro along the finger. If there is nerve injury, the biro will slide a lot more easily than normal. It should be a bic biro used as other biros do not have the smooth surface required. Soft Tissue Injuries
Amputations: PlasticsAny amputations, even if there is only a small part amputated should be x-rayed, dressed, bandaged and elevated. Give analgesia, tetanus cover and, broad spectrum antibiotics.
Wrap the amputated part in moist saline swabs and place in a sealed plastic bag surrounded by ice/water mix at 4 degrees.
Amputations should be referred urgently to plastics. If there is problem obtaining haemostasis, and ED seniors can not help, urgent orthopaedic help may be needed.
Finger pad amputations: PlasticsFinger pad amputations are common, especially in children. If skin loss is <1cm2 without bony exposure it may be allowed to heal with non-stick dressings. Larger areas of loss may require grafting. Even if they are small, these wounds need regular follow up and are best followed up in the plastic clinic.
Crush injuries: UCC Review Clinic or GPCrush injuries often cause “burst” injury of fingertip wounds. They should be cleaned, and then closed as appropriate. Remember the wound is likely to swell, so closure can be difficult.
Most of the time these injuries can be reviewed by the GP or Practice Nurse. If you suspect blunt tendon rupture, they need review in plastics clinic. If the area of crush is significant, plastics must be involved.
High pressure injection injuries: PlasticsRefer for immediate exploration and debridement, even if the injury appears minor.
Pulp Infections: GPRemember to X-ray to look for a foreign object or osteomyelitis. Incise over the point of maximal fluctuence, and send the patient home with oral antibiotics (flucloxacillin) and wound care advice.
Pyogenic flexor tenosynovitis: PlasticsKanavel’s signs: tenderness over the flexor tendon, symmetrical swelling of the finger, finger held in flexion, pain on passive extension
Refer for exploration, irrigation, and IV antibiotics.
Phalanx FracturesDistal phalynx fracture (closed): GP/ plasticsAnalgesia and elevation. Buddy strap for symptomatic relief.
These heal well, and do not need orthopaedic or plastic follow up, unless they are complicated. In children, if the fracture is through the growth plate the injury should be followed up by plastics.
Distal phalynx fracture (open): PlasticsThis counts as a complicated fracture and should be referred to plastics for consideration of exploration.
Simple proximal and middle phalangeal fractures: GPThese should be treated with excellent elevation, neighbour strapping and analgesia. Unless requiring manipulation, they do not need follow up. Make sure you have a good lateral to assess the degree of rotation or angulation.
Complicated proximal and middle phalangeal fractures: plasticsAny angulated phalynx fractures should be manipulated - use a needle-holder or pencil placed adjacent to the web space as a fulcrum. You may need to maintain reduction with a volar slap or a Zimmer splint.
Refer speedily for surgical fixation if reduction is unsatisfactory or can not be maintained.
Phalangeal Dislocations: plasticsAlways X-ray before reduction and then reduce under digital nerve block or entonox with traction and gentle manipulation. Check integrity of the collateral ligaments after reduction. Buddy strap, elevate, analgesia and provide follow up. Metacarpal fractures
The management of a metacarpal fracture depends on which bit of the metacarpal, which finger, and how angulated it is. Elevation is the most important component of treatment!
Metacarpal Head: PlasticsApply a volar slab, encourage elevation, and refer to plastics.
Metacarpal Neck and Shaft: plasticsCarefully assess degree of rotation and then apply a volar slab or ulnar gutter. Encourage elevation. Most fractures are treated non-operatively, especially in the middle and index metacarpal.
Refer acutely for operative intervention if any rotational deformity, more than 5mm shortening or more than 10o, 10o, 20o, 20o of angulation respectively for 2nd - 5th metacarpals.
Metacarpal Base: plasticsCheck lateral x-ray carefully to ensure the carpo-metacarpal joint is not dislocated, as metacarpal base fractures are frequently fracture-dislocations. These are typically unstable and should be treated with a volar slab or ulnar gutter, elevated, and referred to plastics.
Thumb Base fractures: plasticsIntrarticular: Bennett’s (fracture fragment on ulnar side of thumb)
Rolando (fracture fragment on radial side of thumb)
Apply a bennett’s POP (like a scaphoid but thumb abducted) and refer to plastics for speedy operative repair.
Extraarticular: Check dorsal angulation. If angulated more than 30o or shortened more than 4mm, need speedy operative repair. If non-angulated, refer to plastics for follow up.
Thumb dislocations: plasticsReduce thumb dislocations, then immobilise in a scaphoid POP + follow up.
.
Little (5th) MC dislocation: plasticsMay be associated with fracture - refer after reduction for internal fixation.
MCPJ Dislocation: plasticsAfter reduction assess integrity of collateral ligaments. Then immobilise in 15 degree flexion. If failed reduction, refer for open reduction
Other Hand ProblemsVolar plate injury: plasticsHyperextension at the PIPJ injures the volar plate at the base of the middle phalanx without evidence of bony involvement. Examination shows fusiform swelling of the PIPJ with tenderness over the volar aspect. Treat with buddy strapping to adjacent fingers. Plastics review needed to ensure full mobility regained.
Locked Finger: plasticsThis is common in elderly patients with osteoarthritis. There is often no history of trauma. Refer for hand surgeon opinion - do not try to straighten the affected finger.
Trigger finger/ thumb: GPSpecialist to inject steroid injection into the flexor tendon sheath. GP to refer to orthopaedics.
Fight Bite: PlasticsSuspect a fight bite in any patient presenting with wounds on the dorsum of the hand over the index, middle, ring or little finger MC heads of having sustained a human bite, what ever history is given. Many plastic surgery centres will thoroughly irrigate all of these wounds in theatre, so discuss them all.
Reading and References
http://academiclifeinem.com/pv-card-metacarpal-fractures/ http://learning.bmj.com/learning/module-intro/managing-minor-skiing-snowboarding-injuries-primary-care.html?moduleId=5003325&searchTerm=%E2%80%9Chand%E2%80%9D&page=3&locale=en_GB https://gmep.org/media/13991
http://lifeinthefastlane.com/insidious-injury-002/ http://practicalplasticsurgery.org/the-book/ The Pulvertaft Assessment & Management of Acute Hand Injuries (
http://www.pulvertafthandcentre.org.uk/courses.asp?pageId=56 )http://journals.lww.com/em-news/Fulltext/2011/12000/ED_Treatment_of_Flexor_Tendon_Injuries.4.aspx http://bestbets.org/bets/bet.php?id=51
http://www.eatonhand.com/complic/text02.htm http://www.passthefracp.com/Nerves%20of%20the%20Hand.htm
http://bestbets.org/bets/bet.php?id=972 http://bestbets.org/bets/bet.php?id=603 http://bestbets.org/bets/bet.php?id=103 http://bestbets.org/bets/bet.php?id=284 http://bestbets.org/bets/bet.php?id=2205






 It's difficult to separate the radius from the ulnar as you progress up the forearm but isolated fractures can occur. Forearm fractures frequently seen in school aged children after a fall. Adult fractures may be markedly displaced with little or no bony contact between the fragments. ORIF needed
It's difficult to separate the radius from the ulnar as you progress up the forearm but isolated fractures can occur. Forearm fractures frequently seen in school aged children after a fall. Adult fractures may be markedly displaced with little or no bony contact between the fragments. ORIF needed 


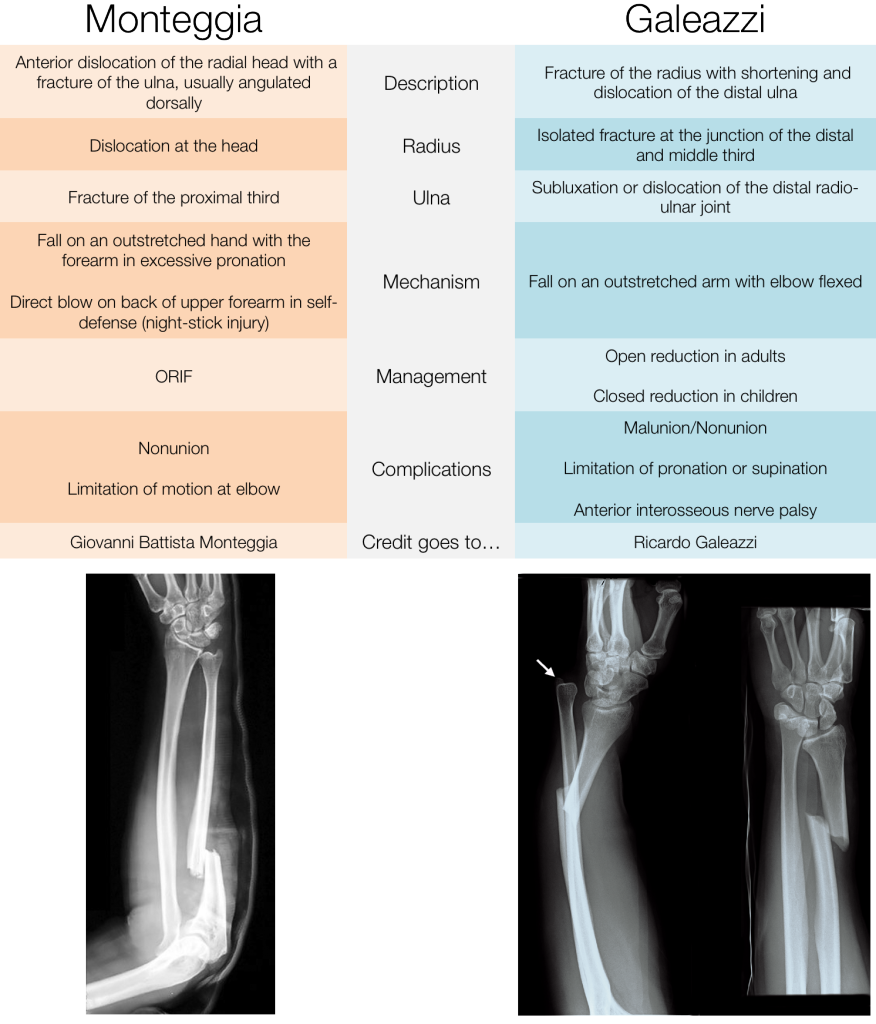

 Radius within 2.5cm of the wrist. Distal fragment angulated to point dorsally.
Radius within 2.5cm of the wrist. Distal fragment angulated to point dorsally.



 The Olecranon is the proximal part of the humerus. It is rare to fracture it. Olecranon fractures usually occur after
The Olecranon is the proximal part of the humerus. It is rare to fracture it. Olecranon fractures usually occur after Radiological Findings
Radiological Findings


